shoulder pain ddx
- folder: MSK
- related: shoulder pain tests, 02 Shoulder
aehesive capsulitis
This patient's clinical features – shoulder pain with decreased active and passive range of motion (ROM) – are most consistent with adhesive capsulitis (AC) (frozen shoulder syndrome). AC can be idiopathic or secondary to underlying conditions such as rotator cuff tendinopathy (most common), subacromial bursitis, paralytic stroke, diabetes mellitus, or humeral head fracture. The glenohumeral joint loses its normal distensibility due to chronic inflammation, fibrosis, and contracture of the joint capsule.
AC typically begins with shoulder pain that is often worse at night. Patients then develop gradual shoulder stiffness (with or without pain) that limits their ability to flex, abduct, or rotate the humerus. The diagnosis is confirmed clinically with >50% reduction in both passive and active ROM in >2 planes (especially external rotation and abduction) compared to the unaffected shoulder. Imaging (x-ray, ultrasound, MRI) is not required for diagnosis but may occasionally be needed to rule out other etiologies of shoulder pain.
Management of adhesive capsulitis (AC) is dependent on the severity of pain and limitation in activity. AC is frequently self-limited, although complete recovery can take up to 6-18 months and residual stiffness is common.
Oral glucocorticoids are not routinely recommended for AC as they provide only temporary relief and are associated with significant systemic side effects. Intra-articular injection is preferred if glucocorticoids are needed. Nonsteroidal anti-inflammatory drugs also provide only temporary relief and have little utility in AC.
Most cases may be managed with resting the shoulder combined with gentle range of motion (ROM) exercises, such as pendulum-type swinging of hand-held weights and walking the fingers up a wall. Patients with significant limitation in function or those who do not improve after 2-3 months of ROM exercises can receive a glucocorticoid injection into the joint; this may be combined with saline distension of the joint space. More aggressive physical therapy may also be considered, either alone or in combination with steroid injection, but evidence for benefit is limited.
subacromial bursitis
Subacromial bursitis typically occurs in patients with a history of heavy lifting or repetitive movements, especially with the arm raised above shoulder level. Patients can develop pain on abduction of the shoulder and restricted active ROM. However, passive ROM should be intact.
rotator cuff tentinopathy
Rotator cuff tendinopathy with a partial or complete tear may cause pain with mildly (partial) or severely (complete) decreased active ROM. However, unless there is concurrent adhesive capsulitis, passive ROM is not affected.
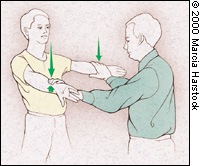 Supraspinatus examination (“empty can” test). The patient attempts to elevate the arms against resistance while the elbows are extended, the arms are abducted and the thumbs are pointing downward.
Supraspinatus examination (“empty can” test). The patient attempts to elevate the arms against resistance while the elbows are extended, the arms are abducted and the thumbs are pointing downward.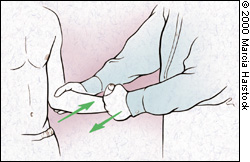 Infraspinatus/teres minor examinatio
Infraspinatus/teres minor examinatio